Disinfected Nurse Shoes Are Still Contaminated, STAND+ (formerly Gales) Study Finds
- Gales+ conducted a nurse shoe contamination study to determine if shoe design/material impacts cross contamination
- They found that in 7 out of 8 shoes, disinfecting the shoes was not enough to prevent cross-contamination
- Gales+ Frontline Nurse Shoes were the only shoe that passed the test

Rob Gregg, CEO of the footwear company STAND+ (formerly Gales), put his life on hold and became a full-time healthcare volunteer after nurses helped to treat his close friend at the beginning of 2020. While working with the nurse innovation group SONSIEL, he soon discovered a crucial need to address the lack of infection control when it comes to footwear.
According to the STAND+ (formerly Gales) website and a 2020 healthcare facility survey, 80% of shoes worn in healthcare environments absorb deadly bacteria. The International Labor Organization also documented that 90% of footwear tested could track deadly bacteria anywhere the wearer goes.
Gregg, also the owner of a luxury Italian footwear company, shut down operations to dedicate his time and energy to designing high-quality footwear for healthcare workers that would be comfortable, safe and bring the spreading of infection in hospitals and homes to a halt.
STAND+ (formerly Gales) footwear, highly recommended by nurses in Nurse.org’s Best Shoes for Nurses list, has given us exclusive access to publish their research study on nurse shoe contamination in hospitals and medical settings. Nurse.org did not receive compensation for publishing this study.

Why STAND+ (formerly Gales) Conducted a Nurse Shoe Contamination Study
Surfaces throughout the healthcare setting, including many high-touch areas in patient rooms like bed tables and bed rails, house bacteria and other sources of infection that can spread via direct or indirect contact. Proper cleaning and disinfection of all contaminated surfaces is crucial to reduce the spread of Healthcare Associated Infections (HAI).
Clothing worn by healthcare professionals is also subject to contamination. Universal precautions, including proper hand hygiene and gloving, help to limit infection transmission, but it’s not foolproof.
Floors are sometimes overlooked as a source of contamination, yet often things like shoes, socks, and slippers come in contact with the floor and are subsequently handled by healthcare workers. Objects like blood pressure cuffs and call bells fall on the floor, too, exposing them to the contaminated area.
Shoes worn by healthcare workers are in constant contact with contaminated floors. According to the researchers, numerous published studies demonstrate that shoe barriers/covers offer inadequate protection of shoes from contaminated surfaces and environments.
Study Objective: Does Nurse Shoe Design/Material Impact Cross Contamination & Can Shoes be Adequately Cleaned?
The study was conducted by Hospital Epidemiologist Victor R. Lange with the objective to answer the question of whether there is a correlation between shoe design/material and increased cross-contamination. Lange sought to determine if shoes worn by healthcare workers can be adequately cleaned and disinfected when soiled or contaminated by blood or body fluids in the hospital and to use the information to help mitigate the transmission of bacteria and infection in healthcare facilities.
Study Methodology
To do this, the researchers enrolled eight nurses working in a community hospital who were educated on infection prevention as part of the hospital's new-hire and annual skills curriculum to ensure competency in proper surface disinfection techniques.
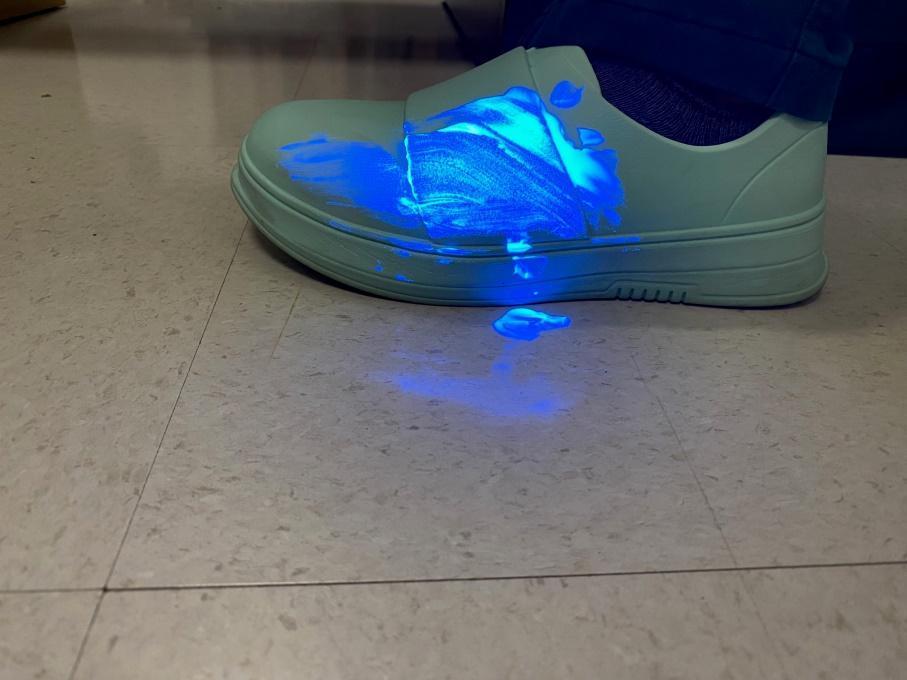
Glo Germ™, a commercially available fluorescent marker and ultraviolet light (UV) to visualize environmental particles, was utilized to study shoe surface contamination after intentionally exposing it to body fluid by a simulated splash with all eight participants.
After visualizing the UV light with the Glo Germ reaction on the simulated splash, participants were instructed to use hospital-provided sanitation wipes to thoroughly clean the shoe surface and allow it to air dry for five minutes. The shoe surface was re-illuminated with UV light after cleaning, and results were recorded based on a scale of 0-5. (0 indicating no removal of Glo Germ and five being complete removal of Glo Germ to the naked eye).
Participants also removed the shoe to evaluate the sock according to the Glo Germ-UV light protocol. Researchers photographed the inside of shoes to visualize the extent of Glo Germ penetration onto the sock.
Key Takeaways
- Disinfecting shoe surfaces was not an adequate intervention in seven of the eight shoes they wore. The study's results were indisputable. Based on the nature of various shoes worn by healthcare workers, disinfecting shoe surfaces was not an adequate intervention in seven of the eight shoes they wore. The researchers believed the contamination was due to the upper component of the athletic-type shoes constructed of materials that could help circulate air and absorb foot perspiration.
- The STAND+ (formerly Gales) Frontline Nurse Shoes were the only shoe that adequately removed Glo Germ from the shoe surface and had no seepage of Glo Germ from the inside of the shoe onto the sock.
- According to researchers, adequately cleaning and disinfecting shoes relies heavily on their materials and construction. The sole in contact with the floor protects the bottom of the foot. While the sole usually has a tread to help with traction, it’s also a source of contaminant accumulation and redistribution during wear.
- Additionally, many healthcare professionals wear “athletic-style shoes” made with nylon or polyester that form to the foot for comfort and provide adequate ventilation. The wicking nature of some of these materials also doesn’t allow for appropriate disinfection, and contaminants can easily leak through and be absorbed into the sock.
- Based on shoe construction and design, the study concluded that seven of the eight shoes failed to be acceptably disinfected after a simulated splash of bodily fluid. Despite hygienic measures, pathogens may persist on footwear even after cleaning with disinfectant.
- Only the Gales+ shoes passed the test. Their construction and design make them easy to clean, preventing the spread of infection in healthcare facilities and reducing the chances that workers will take pathogens home.
| Shoe Brand | Model # | # Exposures to Glo Germ™ | Ability to remove Glo Germ™ from shoe surface** | Transfer of Glo Germ™ onto sock through wicking |
| Asics | Tiger Runner II | 1 | 2 | Yes |
| Brooks | Adrenaline 22 GTS | 1 | 1 | Yes |
| Brooks | Levitate StealthFit 5 | 1 | 2 | Yes |
| Crocs | Classic Clog | 1 | 3 | Yes |
| Gales | Frontline Nurse Shoes | 1 | 4 | No |
| New Balance | ML515V3 | 1 | 1 | Yes |
| New Balance | 327 | 1 | 1 | Yes |
| Nike | Metcon 8 | 1 | 1 | Yes |
What Makes Gales+ Shoes Different, and How Can You Buy Them?
Gales+ shoes are antimicrobial, waterproof, fully bleachable, and machine-washable.
Nurses love them because they provide “cloud-like” comfort during long shifts by reducing pressure on the knees, back, and joints. They have many colors to choose from and are backed by nurse influencer and comedian, Nurse Blake.
You can shop for all their shoes and accessories at Gales+ Frontline Nurse Shoes.
Read the Full Gales+ Shoes Study
Shoe Contamination: Risk Factors Associated With Contaminated Shoes Worn By Healthcare Workers While in the Hospital or Medical Setting
BACKGROUND:
Environmental surfaces in the healthcare environment contain a highly diverse population of microorganisms. Such surfaces can serve as potential reservoirs for these pathogens, often leading to cross contamination through direct or indirect contact.
Contamination of surfaces, including high-touch surfaces in patient rooms (i.e.: over-bed tables, bedrails, etc.) is a known risk factor in contributing to ongoing cross-contamination in healthcare facilities. Therefore, cleaning and disinfection of such environmental surfaces has been of fundamental importance in reducing the potential contribution of these contaminated surfaces in order to decrease risks of Healthcare Associated Infections (HAIs).
According to the Centers for Disease Control and Prevention (CDC), approximately 687,000 patients contracted a nosocomial infection in a United States (U.S.) hospital in 2015, a rate of one out of 31 patients.3 Any person that enters a health care facility contributes to the ongoing contamination cycle. Nearly 40% of shoes in a community setting contain traces of toxigenic Clostridium difficile, a commonly contracted microorganism found in hospital environments.13
Clothing of healthcare professionals are often subject to a high level of contamination by pathogens. The use of universal precautions such as gloving, along with hand washing have been successful in limiting some transfer of foreign pathogens.7 However, although these preventative practices are implemented by clinicians, cross-contamination still occurs. Pathogens that cause Healthcare Associated infections (HAIs) mainly contaminate healthcare professionals when providing care to patients.7
Floors of healthcare facilities are reservoirs for pathogens. One study demonstrated that “hospital floors are often heavily contaminated but are not considered an important source for pathogen dissemination as they are rarely touched. However, floors are frequently contacted by objects that are subsequently touched by hands, (e.g., shoes, socks, slippers). In addition, it is not uncommon for high-touch objects such as call buttons and blood pressure cuffs to be in contact with the floor.” 8
Another study measured the organism load on an Australian surgical unit, subsequently identifying a very high prevalence of pathogens on various sites of floors: 1,854 colony forming units (CFUs) in the main corridor, 2,598 CFU found on bathroom floors, and 1,074 CFU on patient room floors.5 The researchers attributed this finding to shoe contamination, as well as a lack of standard practices for cleaning and personal protective equipment (PPE) to prevent transmission. The role that shoes have in transmitting pathogens that cause HAIs should be better understood.4
The shoes of healthcare workers have often been overlooked as a potential fomite or vector for pathogenic transmission. There may be a correlation between shoe design/materials, and the ability to properly disinfect the shoes thereby increasing the likelihood of cross contamination. Although limited, there are recent studies published that demonstrate a statistically significant correlation between the spread of various pathogens within a hospital environment due to contamination of healthcare worker shoes.
OBJECTIVE:
To determine if the shoes normally worn by healthcare workers allow for proper cleaning/disinfection when potentially soiled/contaminated by blood or body fluids in the high-risk environment in hospitals. To provide further information regarding risk factors attributable to shoes worn by healthcare workers, thereby assisting in further mitigation of consequential transmission of microorganisms.9
METHODS:
This study was a prospective experimental study that measured and evaluated the effect of a purposively applied intervention, involving the contamination of healthcare worker shoes with Glo Germ™ simulated bacteria liquid and illuminating the contaminated surface with a portable Ultraviolet light (uvBeast V3 365nm Mini – Black UV Flashlight – High Definition Ultraviolet)
Glo Germ™ (Flo Germ, Moab, UT) is a commercially available fluorescent marker. It consists of 5 mm particles. It is sold in powder form and oil-based suspension of a melamine copolymer resin.10 It is used in conjunction with ultraviolet light (UV) (black light) which allows for visualization of small particles in the environment. This formulation has been used to educate healthcare workers regarding the proper technique for donning and doffing of PPE and has allowed for the observation that personnel contamination with infectious materials of different kinds can occur.11
The study population was derived through a purposive sample of convenience, including nursing staff working in a community hospital (n = 8). Study participants consisted of nursing staff who received instruction and training on Infection Prevention as part of hospital new-hire and annual skills curriculum. This included verified competency of surface disinfection techniques.
Utilizing the Glo Germ™ synthetic bacteria that fluoresce under black light, the study involved shoe surface contamination from intentional exposure – simulating body fluid splash. Simulated exposure was performed in a manner consistent in all study participants.
1 mL of Glo Germ™ would be drawn into a syringe and voided onto the top of each participant shoe and allowed to sit undisturbed for 1 minute. After the dwell time passed, the shoe surface would be illuminated utilizing the UV light to visualize the location of the Glo Germ™.
The participant was then asked to utilize hospital provided sanitation wipes, wiping the shoe surface thoroughly and allowing to air dry for 5 minutes based on the sanitation wipes Instructions for Use (IFUs). The shoe surface would once again be re-illuminated with the UV light and the result would be recorded based on a scale of 0-5 (0 indicating no removal of Glo Germ™, to 5 being complete removal of Glo Germ ™as visible to the naked eye).
Participants would also remove the shoe, and the sock surface would also be evaluated as indicated in the prior step. Shoes with Glo Germ™ breakthrough onto the sock would also be photographed internally to visualize Glo Germ™ penetration.
RESULTS:
8 study participants voluntarily subjected their footwear to contamination simulation utilizing Glo Germ™ fluorescent marking liquid. After exposure, shoe surfaces would be wiped off utilizing hospital germicidal wipes and allowed to air dry for 5 minutes according to manufacturer’s IFUs. (Figure1 & Figure 4) The residual Glo Germ™ left behind after wiping would be evaluated based on a numerical scale and recorded (Table 1) (Figure 2 & Figure 5)
Study findings also demonstrate a correlation of shoe saturation/wicking of Glo Germ™ fluorescent marking liquid, transferring onto the surface of the healthcare worker’s socks. (Figure 3)
Table 1.
| Shoe Brand | Model # | # Exposures to Glo Germ™ | Ability to remove Glo Germ™ from shoe surface** | Transfer of Glo Germ™ onto sock through wicking |
| Asics | Tiger Runner II | 1 | 2 | Yes |
| Brooks | Adrenaline 22 GTS | 1 | 1 | Yes |
| Brooks | Levitate StealthFit 5 | 1 | 2 | Yes |
| Crocs | Classic Clog | 1 | 3 | Yes |
| Gales | Frontline Nurse Shoes | 1 | 4 | No |
| New Balance | ML515V3 | 1 | 1 | Yes |
| New Balance | 327 | 1 | 1 | Yes |
| Nike | Metcon 8 | 1 | 1 | Yes |
** 0-5 (0 indicating no removal of Glo Germ™, to 5 being complete removal of Glo Germ ™as visible to the naked eye)
Figure 1.

Shoe contaminated with Glo Germ™.
Figure 2.

Shoe after being wiped down using a hospital germicidal wipe.
Figure 3.

Glo Germ™ transfer onto sock through mesh surface of shoe.
Figure 4.
Solid construction shoe with Glo Germ™ splashed to surface
Figure 5.
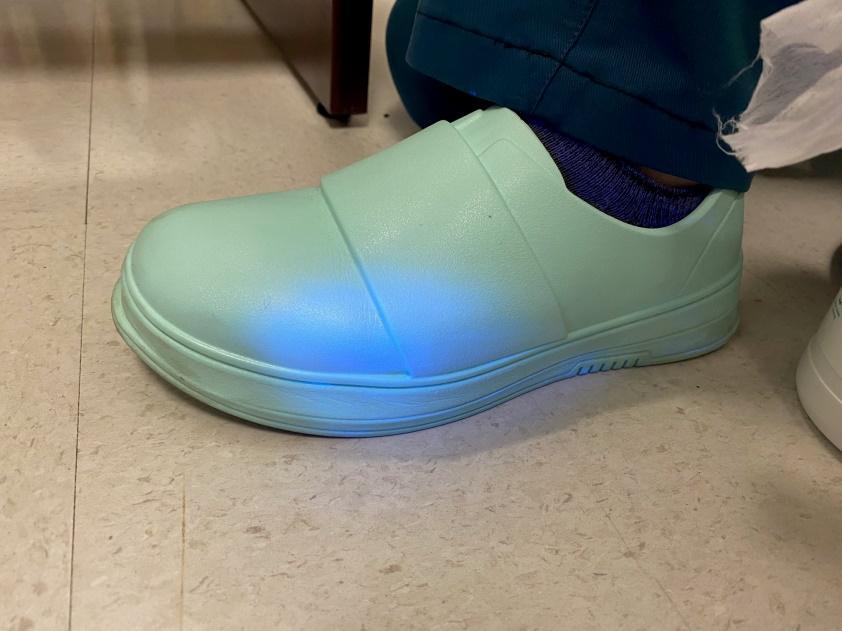
Solid shoe after Glo Germ™ wiped off surface utilizing hospital germicidal wipe.
DISCUSSION
Footwear exposed to the hospital environment is subject to contamination by the unique organism populations commonly found in healthcare facilities. Organisms foreign to the hospital environment may be introduced into these settings via footwear contamination. Therefore, footwear serves as a vector for organism transmission in the hospital environment.
Controlling the spread of infectious organisms is a top priority within the healthcare industry. Sanitization/Disinfection efforts, personal protective equipment, and other measures have been implemented and innovated to promote this aim. Furthermore, numerous published studies have demonstrated that even shoe barriers/covers do not allow for adequate protection of shoes from the contaminated environment.
The longstanding premise of shoe covers worn by healthcare workers is to lessen the risk of shoe contamination and subsequent organism spread. A review of three published studies included in this review tested a hypothesis of utilizing shoe covers, to deter the spread of infectious organisms.2,6,14 In two of the studies, both concluded there were no significant differences between the data collected before and after periods of shoe cover intervention, respective to organism transmission measures.6, 14 Furthermore, the third study conducted found a significantly higher rate of infection during the shoe cover intervention phase as opposed to the shoe phase. 2
Based on these three studies, it can be concluded that the incorporation of shoe covers in a hospital facility does not deter the prevalence of organism transmission. In fact, they may make pathogenic transmission worse.
SHOE CONSTRUCTION
Shoe construction appears to play a vital role in the ability to adequately be cleaned/disinfected. Shoe manufacturers utilize various materials in the construction of their shoe products.
Shoes are generally constructed with three major components; a sole - to contact the floor and protect the bottom of the foot, a midsole - to form the contour and shape of the foot for better fit, and an upper – to enclose the foot securely
The sole of the shoe will usually be treaded to increase the coefficient of friction (static and kinetic) However, it often represents a surface to capture and re-distribute contaminants acquired during wear periods. Shoe soles can be made of material such as leather, polyurethane, EVA, ABS, PVC, and even cork materials may be present in various modern-day shoe construction.
The upper component of the shoe can be of a solid material such as vinyl or leather, or perhaps a composite material. Many of the shoe products worn by professional are traditional athletic or running type shoes.
The traditional “athletic shoe” style is made of high tenacity yarns (nylon or polyester) that easily form to the shape of the foot. Each individual yarn is made of 17 to 34 separate fibers or filaments that form channels which further facilitate air and fluids and also allows the upper to form to the shape of the foot.
During movement and walking, the upper’s pliability facilitates a ‘pumping’ characteristic for flow in and around the foot. The mechanical properties of such materials therefore contribute to further inhibiting or absorbing various contaminants and/or liquids when in contact with the surface of various shoe materials.
Furthermore, through the normal cleaning/disinfection techniques utilized via healthcare workers (i.e. - disposable wipes/cloths), the wicking nature of some of these materials will not allow for appropriate disinfection, furthermore leading to contamination that leads to the sock of the healthcare worker.
CONCLUSION
Footwear worn in hospital settings is a contributing factor to organism transmission. Glo Germ™ simulated bacteria liquid that fluoresce under black light, the study demonstrated that based on the nature of various shoes worn by healthcare workers, surface disinfection was not adequate in 7 of the 8 shoe types worn by the healthcare worker participants. This also accounted for 7 of the 8 shoes leading to sock contamination. These simulated contamination events were likely due to the upper component of the athletic type shoes being made of materials that facilitate air and fluid absorption by virtue of design.
The study can translate to real-world scenarios, in which we can see various organisms being recovered from the intricate surfaces of footwear. This study and subsequent reference review has also highlighted that despite hygienic measures undertaken by healthcare workers, the high likelihood of pathogenic organisms may persist on footwear, despite incorporating surface cleaning/disinfection protocols.
REFERENCES
-
Agarwal, M., Hamilton-Stewart, P., & Dixon, R. A. (2002). Contaminated operating room boots: The potential for infection. American Journal of Infection Control, 30(3), 179– 183. doi:10.1067/mic.2002.119513
-
Ali, Z., Qadeer, A., & Akhtar, A. (2014). To determine the effect of wearing shoe covers by medical staff and visitors on infection rates, mortality and length of stay in intensive care unit. Pakistan Journal of Medical Sciences, 30(2), 272–275 doi:10.12669/pjms.302.4384
-
Centers for Disease Control and Prevention. (2018). Hospital acquired infections: data. https://www.cdc.gov/hai/data/portal/index.html.
-
Clesham, et. al., "Assessment of theatre shoe contamination in an orthopaedic theatre. Author links open overlay panels: Journal of Hospital Infection, Vol. 99, Issue 3, July 2018, pp 299-302.
-
Galvin, J., Almatroudi, A., Vickery, K., Deva, A., Lopes, L., Costa, D., & Hu, H. (2016). Patient shoe covers: Transferring bacteria from the floor onto surgical bedsheets. American Journal of Infection Control, 44(11), 1417–1419. doi:10.1016/j.ajic. 2016.03.020
-
Gupta, A., Anand, A., Chumber, S., Sashindran, V., & Patrikar, S. (2007). Impact of protective footwear on floor and air contamination of intensive care units. Medical Journal, Armed Forces India, 63(4), 334–336. doi:10.1016/S0377-1237(07)80009-8
-
Kanwar, A., Thakur, M., Wazzan, M., Satyavada, S., Cadnum, J., Jencson, A., & Donskey, C. (2019). Clothing and shoes of personnel as potential vectors for transfer of health care– associated pathogens to the community. American Journal of Infection Control, 47(5), 577–579. doi: 10.1016/j.ajic.2019.01.028
-
Koganti, S., Alhmidi, H., Tomas, M., Cadnum, J., Jencson, A., Donskey, C. (2016) Evaluation of hospital floors as a potential source of pathogen dissemination using a nonpathogenic virus as a surrogate marker. Infection Control & Hospital Epidemiology, 37(11), 1374- 1377.
-
Macdonald, L. (2015). Standard infection control precautions (SICPs) literature review: personal protective equipment (PPE) - footwear. Health Protection Scotland, 14, 1-14. 29 https://hpspubsrepo.blob.core.windows.net/hpswebsite/nss/2606/documents/1_sicplrfootwear-v2.0.pdf
-
Oberyszyn AS, Robertson FM. Novel rapid method for visualization of extent and location of aerosol contamination during high-speed sorting of potentially biohazardous samples. Cytometry 2001; 43: 217-222.
-
Osei-Bonsu K, Masroor N, Cooper K, et al. Alternative doffing strategies of personal protective equipment to prevent self-contamination in health care setting. Am J Infection Control 2019; 47: 534-539.
-
Poller B, Hall S, Bailey C, et al. VIOLET: a fluorescence-based simulation experience for training healthcare workers in the use of personal protective equipment. J Hospital Infection 2018; 99: 229-235.
-
Rashid, T., Vonville, H., Hasan, I., & Garey, K. (2016). Shoe soles as a potential vector for pathogen transmission. Journal of Applied Microbiology, 121(5), 1223-1231. doi: 10.1111/jam.13250
-
Sharma, P., Kaur, N., Jitender, & Kaur, M. (2018). Effect of wearing shoes by medical and nursing staff in picu/nicu and bacterial contamination of floors. International Journal of Science and Research, 7(5), 955-956. https://www.ijsr.net/search_index_results_paperid.php?id=ART20182340
